Having had a bit of hiatus in blogging, (it’s almost a year since I last posted!) it’s time to get blogging again and particularly so as I’ve finally made the move to get my own domain on Reclaim Hosting.
I first started blogging here on e-LiME in 2008 and I’ve been struck in the past year by how often I refer back to some of my old posts, both the published ones and those that have remained as eternal drafts! I was never a prolific blogger but I found blogging was a good way to support reflective practice and think out loud. Some of my old posts are full of questions and were an attempt to gain the views of others and often they generated helpful learning conversations on Twitter, others through comments posted on individual posts.
When I moved to a more central University role two and a half years ago I found it quite a challenge to blog. My previous post was an academic one and I think I felt freer to blog and share some of my thinking, Moving to a professional service puts you in a slightly different position and I guess there’s perhaps been a sense of feeling more wary of blogging. The other challenge has been time, I’ve written lots of blog posts in my mind but they’ve never made it to being spelled out on my keyboard. Recently though I’ve realised that I’ve missed blogging, there’s almost something cathartic about it, but I think importantly for me blogging was a way to reflect and support my own personal learning. So I’m back blogging about higher education, open education, the role of technology in learning and teaching and good old medical education. If you want to keep up with posts on my new digital home you’ll find me blogging over on Still Learning on my own domain.
Following the example set by Andrew Coggins who shared his pearls from AMEE 2016 here are some of my AMEE highlights and the things that have left me with food for thought.
AMEE in Barcelona was busy for me as I was involved in running several workshops and I didn’t get chance to get along to all the sessions I would have liked to. A common issue that springs up at AMEE most years is that there are often several sessions running at the same time that you’d like to get along to, this was the case again and I was sorry not to get along to the short communications on self-regulation and self-efficacy and also on learning theory. That said there were sessions that I did get along to and the Twitter stream let you keep an eye on what else was being presented and discussed around the conference.
The opening plenary this year was delivered by Graham Brown-Martin, founder of Learning Without Frontiers who’s travelled extensively looking at schools and education and published Learning Reimagined. Whilst the focus of Graham’s talk was education in the school sector I felt many of the points he talked about had relevance to the higher education context where medical schools sit. We heard from Seth Godin during the talk who highlighted that schools are producing students who can do well in the test rather than students who can problem solve and innovate as well as lead. What struck me was the impact our school system has on shaping the future students entering medical school and in turn future doctors. Typically medical students are fixated on what’s going to be in the exam and our medical curriucla don’t generally focus on developing creativity and innovation in students. Yet there are growing challenges which our graduates will have to grapple with and problems that need to be addressed eg. around caring for ageing populations, antibiotic resistance and how to improve the design of our health services. Graham highlighted how schools need to equip children with the knowledge and skills to reimagine society, to meet the challenges of their generation. Surely this is true for medical education too?
The tendency for technology to be used to perpetuate old approaches to learning based on information transmission was raised and the fact that teaching should not be seen as a delivery system like FedEx was well made. It was refreshing to hear reference to Paulo Friere and critical pedagogy, an approach one doesn’t hear much about in medical education. The notion of the teacher as an artist crafting learning situations for students was also mentioned, which resonated with John Sandars’ comments in our pre-conference workshop on developing blended learning approaches earlier in the day.
Graham also made reference to Seymour Papert and constructionisim – learning as a reconstruction rather than transmission. This is an approach I’ve adopted in an SSC we run – The Doctor as Digital Teacher – where creativity is very much the focus as students create a digital learning resource. My take home from Graham’s plenary was that we need to be doing more to foster and nurture the creativity of our students in medicine. Locally we’ve been developing links with our design school and I wonder if we will start to see more medical schools doing similar. I’ve been particularly struck by the approach that the new Dell Medical School in Texas which is” including a leadership-focused year of self-directed study, a team-based curriculum, and a first-of-its-kind Design Institute for Health, a joint collaboration between the Dell Medical School and the College of Fine Arts, developed to apply design thinking to health care challenges and innovation”. Perhaps this is a theme we might see more of in future AMEE meetings. You can catch up with more from the plenary on the Storify of the tweets that Graham Brown-Martin has published.
Barcamp
My next AMEE highlight was the Barcamp which ran on Monday afternoon. The Barcamp was a new concept for AMEE and it ran across two workshop slots with a focus on technology and informal learning and it proved a rich learning experience on a number of different levels.
The key feature of a Barcamp is the participation of all participants and everyone was invited to suggest topics, questions, or outline problems that they wanted to explore and discuss. The atmosphere was relaxed and informal and there was no shortage of suggestions for us to consider.
The topics were narrowed down as everyone casted their allocated three votes and very quickly about 14 issues were selected and scheduled in to a series of 4 discussion sessions. With a wide range of participants from different continents and working in different medical education contexts we explored topics such as design-based research, the use of social media in learning, recording infromal learning and analytics, addressing the challenges of rigid IT cultures in delivering medical education. The conversation was rich and thought provoking and I think we all learned from each other’s experiences and collective wisdom. I left the session reminded of Alvin Tofler’s quote that, ‘the illiterate of the 21st century will not be those who cannot read and write, but those who cannot learn, unlearn and relearn”. I felt that the Barcamp helped me in that process of unlearning and relearning some approaches to tackle issues around culture in my organisation.
Everyone had a take home message from the BarCamp and I think the one from Laura Bowater is one that many of us would echo, the session gave us time to think, something we have precious little time for in our day to day work.
Feedback from one particpant at #5S#amee2016 sums up what's been great about #ameecamp session – been a joy to have time just to think!
The Barcamp session was run by the Learning Layers project team who as part of an EU funded project have been looking at supporting informal learning in the workplace. The team have also been developing a toolkit and new app the Learning Toolbox which allows you to create learning stacks and share them with your students/trainees. I think the toolbox has great potential and I’m hoping to explore how we might be able to try it out in a number of contexts back in Dundee and not just in medical education. I’m also seeing lots of potential to reuse the Barcamp format in teaching, curriculum development sessions and also as a precursor to a health and social care design hack that we’re planning to run.
The last thing to mention about the BarCamp were the Joy cards which were shared to acknowledge infromal learning.
A number of us received these cards and I’m looking forward to passing on mine to on. The idea behind the Joy cards is that you can record receiving one online with details of who gave it to you and why and where and then over time you can follow the journey of the card. This is such a simple but effective idea and again it’s something which could be adopted more widely in medical education. It was encouraging to receive one and in many ways it reminded me of the wonderful #FOAMed cards that a good number of us have received anonymously through the post.
Talking of #FOAMed as Andrew Coggins has mentioned in his post there was little mention of it in any of the sessions and it didn’t feature as much as it has in previous years in the Twitter stream. For those unfamiliar with FOAMed it stands for free open access meducation and was coined as a concept at ICEM in Dublin in 2012. FOAMed has been adopted as a hashtag in social media spaces across different medical specialties with particularly strong representation in emergency medicine and critical care as well as radiology and paediatrics. Social media channels have effectively supported the development of a community of practice and learning collectives around FOAMed and medical education more generally. This illustration from Tanmay Vora on conversation and sharing as the currency of social community nicely sums of the essence of how I see the FOAMed community works.
I mention all of this beacuse FOAMed is very much a conversation and I think one of the areas that AMEE hasn’t quite cracked is how to keep the momentum on discussions beyond the physical conference and extend the community into the virtual space. Maintaining those conversations would be particularly helpful to the ‘Point of View’ sessions, which were a welcome addition to this year’s AMEE, and a big shout out to Laura Bowater who outlined the need to reframe the antibiotic resistance crisis and address it in our curricula. In the same session was a point of view from Anita Ho from Singapore touching on digital professionalism and the need for positve role models against a backdrop of medics being strangers in a strange land when it comes to online spaces. This for me acentuated the ongoing apparent lack of awareness of FOAMed in the wider medical education community and the countless positive role models there are in the digital landscape invovled in FOAMed and beyond. It would be good to see AMEE conisder giving plenary stage time to one of the well established names in the FOAMed MedEd community.
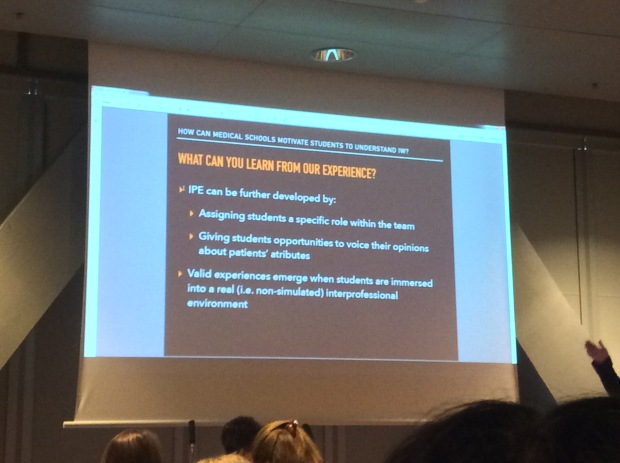
Moving onto interprofessional learning (IPL) there were some super short communications in session #8O. The importance of authenticity in IPL was highlighted by Tineke Westerveld and the presentation by Brazilian medical student Daniel de Oliveira outlining how medical and other health care students work as part of the clinical team in a heart failure clinic proved a great example of authentic learning. Daniel framed the students’ learning in the context of a community of practice and situated learning and urged the audience to include students as part of clinical teams so that they are emmersed in authentic learning. His plea resonated with what I hear many of our students say about IPL, they are always quick to highlight that they will be working in teams with other healthcare professionals yet their expereince of IPL so often seems contrived and unauthentic.
A last highlight to share was Seán MacPherson, the singing haematologist from Otago Medical School, teaching haematology through catchy songs. The example below is a song about anaemia.
Whilst Seán didn’t have hard evidence of the effectiveness of learning medicine through catchy songs the anecdotal indications were that students found them useful way to remember key information and on the VT they mentioned sitting in exams and singing through his songs to recall information. Seán drew parallels with those annoying jingles from adverts that we can’t get out of our heads and we know all the words to. To prove the case he started a rendition of the Shake n Vac and I have to confess I was one of the many that could join in word for word!!
So that wraps up another AMEE. As always it was great to network and meet up with old friends and colleagues as well as to meet and make new friends. I’m looking forward to following up on some of the conversations and to hopefully catching up with others again next year.
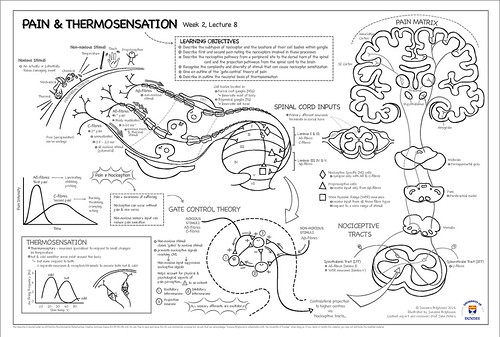
Over the past few years at Dundee we’ve had growing opportunities to work with our colleagues in medical art and suggest project ideas to students studying the Masters programme. There have been some great projects over the years with students developing learning resources, creating comics to support patient communication and exploring the potential of 3D printing to help surgeons. With a long standing interest in the potential of sketchnotes to support student leanrning and in particular revision I’ve pitched a project idea around sketch notes for a couple of years but it’s never grabbed anyone’s attention. This year I floated the idea again and suggested a focus on neurology teaching given that many medical students seem to find this a challenging area of medicine and I was delighted when Susanna Brighouse took on the challenge. First off Susanna created a sketchnote based on a lecture on pain and thermosensation and is with all our student developed resources it was peer reviewed by one of our academics. She produced different versions including one that could be coloured in and labelled by students to support revision.
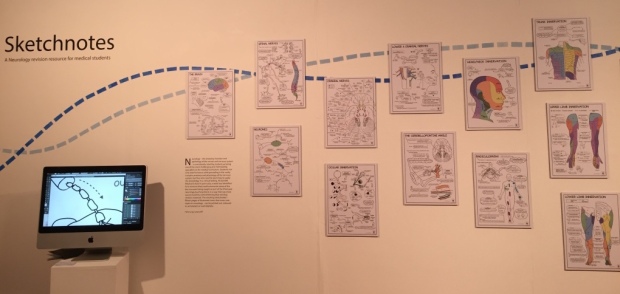
Following positive feedback Susanna went on to make sketchnotes the focus of her Masters project and produced a further 15 sketchnotes based on a series of neurology lectures covering topics such as the anatomy of the spinal nerves, body innervation maps and radiculopathy. Feedback on the sketchnotes from medical students identified that they would make most use of them to help revision. We hope to share these further sketchnotes soon.
Alongside with Susanna’s project there were a few others with a medical education focus where the students had worked closely with Dr Richard Oparka our pathology teaching lead. Two of the projects were super animations, first up a delightful video on the phases and main components of the cell cycle by Cristina Sala Ripoll, which Richard will be using in his teaching with 1st year medical students in a few weeks time. The video highlights the the different phases of the cell cycle that lead to cell division and includes some of the cellular components involved in them.
The second animation comes from Elvire Thouvenot-Nitzan and gives an overview of apoptosis looking at the important role apoptosis plays in growth and development as well as removing DNA damaged cells. It goes on to show how the activation of the caspase cascade occurs in each external and internal signalling pathway and ends with a glimpse of cancer cells and their ability to block apoptosis.
The fourth project I want to showcase is Anna Sieben’s3D epithelium. Anna, who’s a doctor, has created a fantastic teaching resource for medical students on epithelium which links to the virtual microscope used in teaching at Dundee. Students can select to look at the epithelium in different body organs and explore the structure and function of these different tissues through a series of 3D models. I’ve embedded Anna’s model of the epithelium of the skin from sketchfab below. You can 3D print these models from sketchfab and Anna had a wonderful display of these at her degree show.
There’s a lot of focus on technology enhanced learning in medical education and higher education at the moment but I get the impression it’s rare to find medical artists in elearning teams. At Dundee we’re very lucky to have two medical artists in Annie Campbell in medicine and Emily McDougall in dentistry but we don’t have similar posts at the moment in the central elearning team or in other schools. Much of the work that Annie and Emily produce is shared as OER and FAOMed so that others can reuse these resources to support medical and dental education.
Susanna, Cristina, Elvire and Anna are four super talented medical artists and I hope they get snapped up with job offers from other medical or dental schools. I’m looking forward to following their work in the future.
This week is Open Education Week so it seems appropriate to share some work recently completed by one of our Year 3 Medical Students at Dundee as part of our 4-week SSC The Doctor as Digital Teacher.
I’ve blogged before about our SSCs which see medical students developing their digital teaching skills and creating learning resources. Over the years we’ve seen a range of different learning resources developed including online tutorials, iBooks and videos. The students are always very creative and they’ve developed some excellent resources. We only had one student on the latest run of the SSC and I was a bit concerned that we couldn’t offer the same learning experience we usually do when we have five or six students. Thankfully this doesn’t seem to have been the case and our student, Zoe, seems to have enjoyed the experience and has produced a super series of videos on the anatomy of the larynx.
Central to the videos is a 3D model of the larynx which our medical illustrator Annie Campbell worked up as a derivative from content from the Japanese-based BodyParts3D database. We’ve shared this model on SketchFab so that it can be used as OER in other teaching resources.
The videos that Zoe’s created based on this model together with other content that she created, including her own hand-drawn tutorial are all posted up on Vimeo and you can view them here.
Part 1 – Anatomy of the larynx: Cartilage structures
Part 2 – Anatomy of the larynx: Membranes and muscles
This talk from John Seely Brown is 3 years old now but still much food for thought. Seely Brown’s book on ‘The New Lanscape of Learning‘ (co-authored with Douglas Thomas) is one that I suggest to my SSC students to read and review and it always gets a posiitve response. However the students that present this book always highlight that the curriuclum doesn’t particularly embrace these new landscapes of learning and they question whether we are preparing the for the change they will constantly face when they graduate. So after some quick reflection I’m left thinking are we helping to prepare our students to develop their participatory learning skills along with their self-directed and self-regulated learning skills. With the growing trend of viewing students as consumers and spoon feeding is it time for us to start innovating more in our teaching and to become entrepreneurial teachers if we want entrepreneurial learners?
I’ve not got a good track record with MOOCs, I sign up for them, start a few, lurk a bit but invariably don’t finish them as I never seem to have enough time to commit to them. Last year I managed one post on #rhizo14, the other week I spotted that #rhizo15 was starting up so here goes let’s see if I manage more than one post this time round!
For the first task we’ve been asked to think about building learning subjectives and how we design our own learning when we don’t know where we’re going. I’m not sure if I have specific learning subjectives for #rhizo15 but the concept of subjectives brought back to mind the final year of my degree.
Thinking back to my undergraduate student days I can’t really remember having learning outcomes, there was a sense that we’d be assessed on what was covered in the lectures, labs and practicals. I’m sure there will have been course objectives and outcomes but I don’t recall them being explicit or communicated at the start of teaching sessions in the way they are now. Was this a bad thing? After some of my peers complained that they couldn’t hear one of our lecturers he pitched up at his next lecture making it clear that if we wanted to get a decent class of degree then we’d have to do more than regurgitate lectures in our finals. He went on to say we should be doing 10 hours reading per week per module to supplement the lectures. This struck a chord with me and it’s something I’ve reflected on quite a bit over the past few years as I’ve pondered whether our use of technology in higher education has led to spoon feeding students. I didn’t do 10 hours reading per module but I remember reading more round topics that particularly interested me. Certain things spark off a light in your mind, and you pursue your curiosity, or you want to find the information that will help you solve a problem.
In medicine it sometimes seems that students are almost like slaves to learning outcome and objectives, so much of their learning is driven by assessment. The one opportunity they have to break the tyranny of objectives is when they choose their student selected components, they can propose their own 4 week module and set their own objectives. It’s a bit like when you’re at primary school and you all get to pick a topic to explore and create your own topic book. There are things that standout and almost glisten as they grab your attention and stimulate your interest and curiosity. You get drawn to question and explore as they lead you to discover a whole series of other interesting things and take you down paths you’ve never been down before.
I’m not sure what my learning subjectives are but there are things that I’ve been thinking about the past few months including an exasperation around the concept of minimum standards in VLEs and the fact that so often when it comes to technology in higher education there seems to be tunnel vision and a lack of joined up thinking. I’m not sure if these directly relate to the whole concept of rhizomatic learning but perhaps #rhizo15 might serve as a catalyst to help me put aside some time to think and explore and unpick the things that are glistening and catching my eye.
Technology enhanced learning (TEL) is playing a growing role across the continuum of healthcare professions education supporting both formal and informal learning. Virtual learning environments, e-portfolios, e-assessment, online learning and apps are all features of the TEL landscape. Social media is also supporting learning conversations via hashtags like #FOAMed, #ecgclass, #wenurses etc and hosting videos and podcasts on blogs and YouTube. There’s lots to like in the world of TEL in healthcare professions education but there are also frustrations. Frustrations about the clunkiness of institutional learning tools, the barriers to accessing resources from within an NHS setting, the lack of the right sort of apps to support mobile learning. Alongside these problems there are also lots of ideas of how to improve things and make things better together with dreams of how to present and develop content in new more imaginative and effective ways. But these ideas can sometimes lead to additional frustration as indviduals aren’t sure how to turn their ideas into a reality. To help address this NHS Health Education England and the Higher Education Academy are teaming up to run a healthcare professions education hack day – #hetelhack – in Leeds on 7-8 March.
#hetelhack is hoping to build on the success of NHS Hack Days, which have attracted individuals from across the healthcare professions together with patients and developers and coders. The most recent NHS Hack Day in Cardiff is a great example of the creativity and innovation that happens at these events.
Workshops at ASME and AMEE last year highlighted that many of us involved in healthcare professions education face similar issues. Som eof the things that educators and students alike are looking for include
that elusive intuitively designed e-portfolio solution
how we might be able to use technology to make topics like ethics more interesting and engaging
a learning repository that looks more like youtube or slideshare
how we can use tehnology to support the role that patients can play in healthcare professions education
how we might use immersive environments and virtual reality to support developing skills in team working and situational judgement/awareness to help improve patient safety
ways to effectively use 3D printing to support learning
an application that supports collaborative learning
a content authoring app you can quickly and easily use to author and create a short piece of learning that outputs as HTML5
#hetelhack provides an opportunity for individuals to come together and work together over a weekend with coders and designers to solve some of the problems we face or to explore a new idea and be creative. This is the first NHS focussed hack event which has a focus on education and one of the hopes is that we can start to build a network which can also take the ideas that emerge from the hack and collaborate to see them developed further.
There’s been a lot of interest in the #hetelhack but there are still spaces for developers, coders and designers so if you’re free that weekend come along to Leeds.
For more info on #hetelhack and to sign up visist the NHS HEE webiste.
Here’s the second of my post AMEE blog posts which focuses on the pre-conference workshop I ran with John Sanders from the University of Sheffield on ‘How to create personalised learning opportunities in the information age: Essential skills for the 21st century teacher’. John kicked off the workshop looking at why we might personalise learning and some relevant learning theories and how technology is being used to personalise learning.
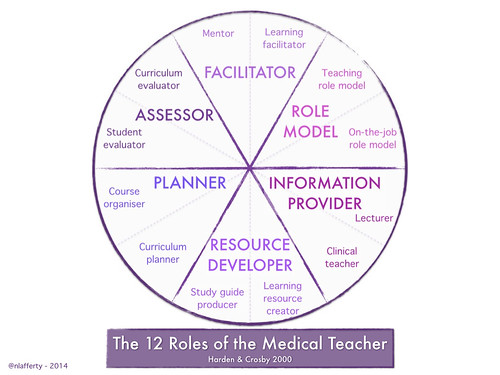
I went on to give a quick overview of how I’ve been using technology to support my own learning and talked about some of the elements of my personal learning environment (PLE) and how I’ve built a personal learning network (PLN). I talked about how this related to my ongoing learning in relation to professional development and the 12 roles of the medical teacher outlined by Crosby and Harden (1) back in 2000. Whilst their focus is on medical education a good number of these roles apply to lecturers whatever their discipline or subject area in higher education.
You can see my slides below which walk through my journey of using social media including blogs, Twitter and the emergence of free open access meducation – FOAMed.
For those of us who’ve been inhabiting digital landscapes for sometime the concepts of PLEs and PLNs are nothing new but for some these are new terms. In the lead up to the conference I was struck by a blog post by Martin Weller asking the question ‘Why don’t we talk about PLEs anymore?’. I think Martin is right, there’s less discussion these days on Twitter and in the blogosphere about PLEs than there was 5 years and I posted this comment on Martin’s blog with some of my thoughts on why this might be.
I wonder if it’s also dropped off the radar slightly because personalised learning is talked about much more rather than personal learning. Much of this is perhaps being driven by the attention on learning analytics and how this can be used to support personalised learning. Along with MOOCs and the flipped classroom, learning analytics seems to be one of the big buzzes (hypes?) in education. I do wonder whether this is a good thing and whether we should actually be focusing more on personal learning so that students develop the skills to become lifelong and wide learners.
I picked up on these themes in another section of the workshop and made the distinction between ‘personal’ learning which is made by and for oneself and self-organised and managed versus what seems to be the current trend around ‘personalised learning’ which to me seems to have become more about learning being customised for individuals and linked to machine learning. Learning analytics seems to be the big driver here and whilst I can see that this can all help support student learning I do have concerns that this is technology spoon feeding students rather than encouraging students to become independent self-directed and regulated learners. Once our graduates are in the work place they have to take personal responsibility for their own personal development and lifelong learning, I’m not sure learning analytics are going to be prescribing learning pathways for them in the world of work (but who knows MOOCS might have taken over the world and this will be the future!).
John went on to look at the importance of both students and teachers having the digital, information and learning literacies to be able to personalise their own learning. He also highlighted that teachers need to have the skills to be able to design learning activities which provide the appropriate scaffolding for students to develop their own personal learning approaches. I think we still have a way to go with teachers developing these skills and the continued reliance on the walled garden of the VLE perhaps doesn’t help. There have been several posts over the past few days about VLEs/LMSs talking about why we’re sticking with VLEs which if time permits I’d like to respond to but in essence I think they kind of miss the point. I think these posts also provide a further answer to Martin Weller’s question about why no one is talking about PLEs anymore, which I think is a real shame.
Within the medical education and health care professions world there is still some scepticism around the use of social media for learning, not least from students who make great use of facebook to support collective learning in their year and study groups but don’t connect much beyond that. There are growing communities around #FOAMed, #WeNurses, WePharmacists etc and there’s a nice editorial by Moorley and Chinn (2) in the Journal of Advanced Nursing looking at using social media for continuous professional development. Closer to home I was interested to see that NHS Education Scotland (NES) have teamed together with the The Institute for Research and Innovation in Social Services (IRISS) to make this video on building your personal learning network.
The press release that accompanied the launch of this video included a great quote from Malcolm Wright who’s the Chief Executive of NES. He said:
‘The social use of knowledge is an important strand of the Knowledge into Action strategy which aims to make finding and using knowledge a routine part of everyday work. By social use of knowledge we mean the tools, techniques and skills that connect people so that they can share experience and find ways of applying knowledge.
We know that published evidence does not translate into practice until people start talking about it and sharing practical examples. Social networking tools such as communities of practice, Twitter and Yammer can play a vital role in this socialising process.’
If you walk the online corridors of #FOAMed this is exactly what you see, personal networks talking over the latest evidence, guidelines, critically appraising them. Senior medics serving as virtual mentors to new doctors and students. With organisations like the NHS recognising the benefits of PLNs perhaps we can start to get PLEs talked about again.
Back in February I blogged about attention and and whether students were checking out of the flipped classroom. In the post I mentioned the work Howard Rheingold has done around attention literacy and videoing one of his classes and then subsequently only allowing one or two students to take notes on laptops in his classes.
Several months on I continue to mull over these issues and so probably no surprise that a tweet linking to a piece on Medium from Clay Shirky outlining why he’s asked his students to stop using laptops and mobile devices in his classes caught my attention. Shirky has banned the use of laptops in class unless they are required and in the piece he explains his rationale. He says:
Over the years, I’ve noticed that when I do have a specific reason to ask everyone to set aside their devices (‘Lids down’, in the parlance of my department), it’s as if someone has let fresh air into the room. The conversation brightens, and more recently, there is a sense of relief from many of the students. Multi-tasking is cognitively exhausting — when we do it by choice, being asked to stop can come as a welcome change.
So this year, I moved from recommending setting aside laptops and phones to requiring it, adding this to the class rules: “Stay focused. (No devices in class, unless the assignment requires it.)”
Shirky goes on to outline the problems with multi-tasking, including the long term negative impact it can have on declarative memory. He says:
People often start multi-tasking because they believe it will help them get more done. Those gains never materialize; instead, efficiency is degraded. However, it provides emotional gratification as a side-effect. (Multi-tasking moves the pleasure of procrastination inside the period of work.) This side-effect is enough to keep people committed to multi-tasking despite worsening the very thing they set out to improve.
On top of this, multi-tasking doesn’t even exercise task-switching as a skill. A study from Stanford reports that heavy multi-taskers are worse at choosing which task to focus on. (“They are suckers for irrelevancy”, as Cliff Nass, one of the researchers put it.) Multi-taskers often think they are like gym rats, bulking up their ability to juggle tasks, when in fact they are like alcoholics, degrading their abilities through over-consumption.
Shirky doesn’t say how his students have taken to this laptop ban though he does highlight that some students will opt of paying attention anyway (something which has always happened anyway even in the days when we didn’t laptops).
Has Shirky been too radical? It would be interesting to hear what lecturers and students think about banning laptops. Is anyone else thinking of banning laptops or already done it. How has that gone down with students.
Last week I was at the annual AMEE conference, which is probably the largest international conference in medical education attracting delegates from across the health care professions and the continuum of education. It also has a reasonable amount of engagement from students and it was great to see so many students presenting both posters and short oral communications. I’m hoping to write a few posts following on from last week and this one is the first in the series with some notes on the symposium I took part in on ‘Creating effective learning with new technology in the 21st century: the importance of educational theories’. Here’s the abstract for the session:
There is an increasing variety of technology available to the 21st medical educator, from social media (such as Twitter and You Tube) facilitating free open access education (FOAMed) to large knowledge repositories and simulations to Massive Open Online Courses (MOOCs). The challenge for all medical educators is to resist the temptation of adopting the latest technology without considering how the technology can be used to facilitate effective learning. This symposium will offer participants a range of established and newer educational theories, from multimedia design and deliberate practice to ecology of learning and connectivism, and illustrate how these theories can critically inform the use of technology to create effective personal and collaborative learning. Participants will have the opportunity to consider the extent to which they currently use theory to create learning opportunities with technology and to explore how they can produce innovative learning with technology by the use of newer theories.
John Sandars, Director of Research at the School of Medicine, University of Sheffield chaired and introduced the symposium and started off by sharing Jean Marc Cote’s vision of a 21st century school from 1901. John went on to outline the importance of the role of the instructor (a theme which was revisited in the discussion) and the need to think about both educational philosophy and theories when designing an instructional approach.
John went on to introduce the four co-presenters in the sympoisum and the topics we’d be covering. First up was Pat Kokatailo, Professor Of Paediatrics at the University of Wisconsin who looked at ‘What type of learner do I want?‘ Pat focused on John Dewey and his core beliefs of the teacher as a facilitator or guide, presenting content in a way which enabled the student to relate to prior experience and engage in active inquiry based learning. She went on to detail how Dewey had informed Flexner and him advocating small group and hands on teaching and how this in turn informed Schon’s reflective practice. Pat went on to talk about what kind of learners we want in medical education, a theme picked up in my presentation and we both highlighted the need for students to develop into independent life long learners who were active and inquisitive and knew where to find information. The role of technology was then considered in how it could be used to develop inquiry by designing activities that encouraged self-direction, promoted interactive activities that also provided feedback to students.
Next up was Goh Poh Sun from Yong Loo Lee School of Medicine in Singapore who presented on ‘Designing effective individual learning’. You can take a look at Poh Sun’s presentation on his Designing effective individual learning blog and the further resources he’s posted on Padlet. One of the themes of Poh Sun’s talk was cognitive load and multimedia learning theories which Richard Mayer has written about extensively.
I then went on to my slot where the focus was on social learning and you can take a look at my slides below.
My main focus was on communities of practice, networked learning and connectivism. There are clearly others such as Bandura’s social learning theory but there’s only so much you can say in 10 minutes. These theories are inter-related and can be used as lenses to gain perspectives on social learning and help develop frameworks to support the design of social learning activities.
Finally Rakesh Patel of the School of Medicine, University of Leicester went to provide a helpful overview of Emergent theories for effective learning. Rakesh’s focus was learning in the clinical and work-based setting and he emphasised the need to prepare our learners for the fast-paced and ever changing workplace that they will practise in. The importance of developing and being able to assess clinical reasoning skills was highlighted and the role that technology might play n helping to identify gaps in student knowledge as well as supporting feedback.
The educational theories outlined by Dewey, Vygotsky, Mayer, Lave and Wenger seemed to weave together through the presentations and it’s clear to see their relevance when designing effective learning with technology. What was clear from the 45 minutes of discussion is the need to explore these further and develop frameworks to support the design of effective learning approaches. Too often our use of technology in learning and teaching has been technology lead, we’ve learned about a new technology and want to use it rather than thinking about what our students need to learn, what skills we want them to develop and how that can best be achieved. The importance of the teacher came through time and time again from the audience and it’s we that need to be the agents of change. With that in mind I’d recommend having a look at this paper by Kirkwood and Price ‘Missing: evidence of a scholarly approach to teaching and learning with technology in higher education‘.
You can gain a further insight into the session by checking out the Storify which includes links to resources and live tweets from the Symposium just click the link below.